Dr. Kai-Nan An Presents
本コンテンツは、第36回日本ハンドセラピィ学術集会でKai-Nan An先生によるご講演内容をおまとめ頂いたものです。
広く日本のハンドセラピストに共有してほしいというAn先生のご意向により、特設サイトを作りました。
An先生は、各論文を掲載することもご許可をいただきましたが、著作権の懸念もありましたので、無料で閲覧できる論文はそのサイトへのリンクを、有料のものは文献情報にリンクさせていただくことにいたしました。
我々ハンドセラピストにとって非常に有益な情報ですのでぜひご利用ください。
The hand plays a crucial role in most daily activities, making it highly susceptible to injury compared to other parts of the musculoskeletal system. Wrist and hand injuries are some of the most common occupational disorders, encompassing conditions such as carpal tunnel syndrome, trigger finger, and tendonitis. Moreover, wrist fractures are the most prevalent type of fractures in the human body. Due to the hand and wrist's complex structure and their vulnerability to injury, the fields of hand surgery and therapy are of utmost importance. The biomechanics of the hand and wrist—encompassing the relationship between anatomy, structure, and function—is the foundational science behind modern hand surgery.
Over the past half-century, the biomechanics of the hand and wrist has garnered significant attention. Numerous experimental and analytical studies have been conducted to improve the understanding of functional anatomy, with the goal of targeting specific disorders and injuries for prevention, diagnosis, and treatment. The principles and technologies derived from these studies can be highly beneficial for hand therapists in their clinical practice.
Mechanics is the scientific discipline concerned with the interactions of force and motion, while biomechanics applies the principles and methods of mechanics to biological systems. Mechanics can generally be divided into kinematics and kinetics. Kinematics involves the study of displacement and motion without focusing on the causes of these movements, whereas kinetics examines the forces responsible for initiating those movements.
This paper will first explore the kinematics of the hand and wrist. It will cover the general movements of the hand and wrist, the specific articulations between the bony structures at each joint, and the anatomical structures responsible for the patterns of motion and joint stability. Clinical implications and applications will also be discussed. Following this, the kinetics of the hand and wrist will be examined, beginning with an overview of the hand's functional strength, followed by an exploration of internal forces, such as joint reaction forces and tendon-muscular forces. Both experimental methods for direct assessment and measurement, as well as the theoretical principles of biomechanics developed and utilized in the past, will be included in this discussion.
This manuscript provides only brief descriptions of the related concepts, principles, methodologies and clinical applications. More details, if interested, could be found in the attached papers with hyperlink to the references cited.
1. Hand Motion
Assessment of hand motion can be accomplished by describing joint motion or the space covered by a specific point on the hand. Describing joint motion is relatively straightforward for planar movements, such as those at the interphalangeal joints, which have one degree of freedom. However, it becomes more complex for non-planar movements, such as those at the metacarpophalangeal joints, the carpometacarpal joints, and the wrist joint.
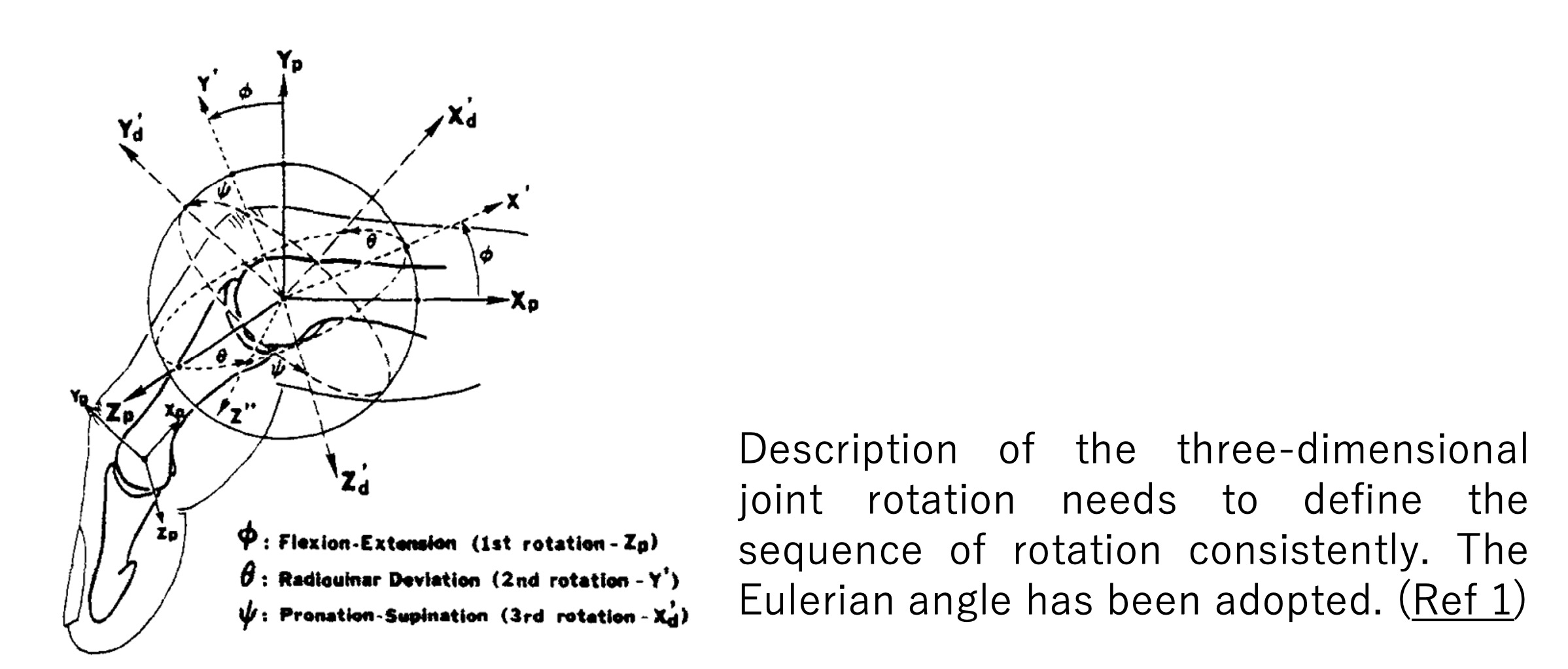
For three-dimensional joint rotation, the description is theoretically sequence-dependent. In other words, the sequence used to describe joint rotation must be specified and agreed upon; otherwise, inconsistent values will be encountered. In hand biomechanics, the Eulerian angle description has been adopted. The sequence of joint rotation is generally first flexion-extension, followed by abduction-adduction or radial-ulnar deviation, and then axial internal-external rotation, if applicable. (Ref 1)
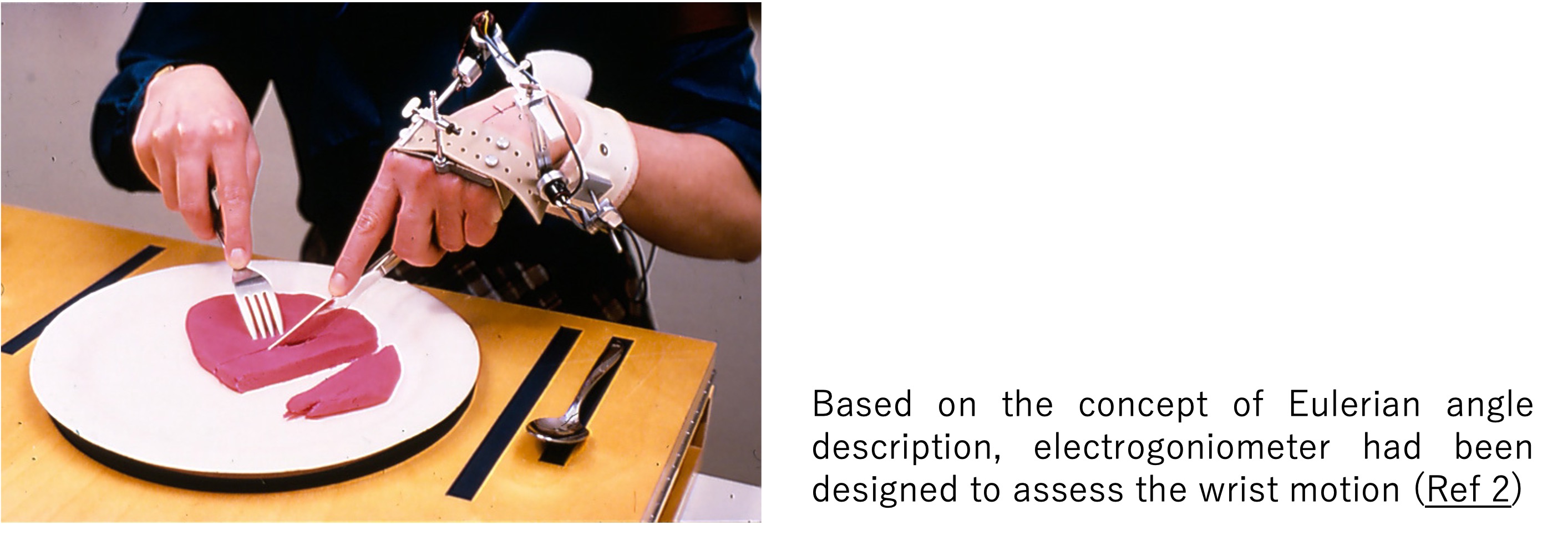
 Experimentally, several approaches have been developed to assess hand joint rotation in both static and dynamic conditions. A hand-held goniometer is commonly used for static joint angle measurements. An electronic goniometer, based on the gimbal system, has been designed to assess wrist motion in flexion-extension and radial-ulnar deviation continuously. The minimum range of wrist motion required for daily activities has been studied (Ref 2).
Experimentally, several approaches have been developed to assess hand joint rotation in both static and dynamic conditions. A hand-held goniometer is commonly used for static joint angle measurements. An electronic goniometer, based on the gimbal system, has been designed to assess wrist motion in flexion-extension and radial-ulnar deviation continuously. The minimum range of wrist motion required for daily activities has been studied (Ref 2).
 Video-based motion systems have also been adopted for assessing hand motion. For example, finger movements in piano playing have been evaluated using such a system (Ref 3). The movement of the fingers associated with the rehabilitation of trigger finger has also been studied. A specific movement pattern was found to be beneficial in reducing tendon tightness and improving tendon gliding. In this study, the space covered by the fingertip was also used to assess treatment effectiveness. (Ref 4)
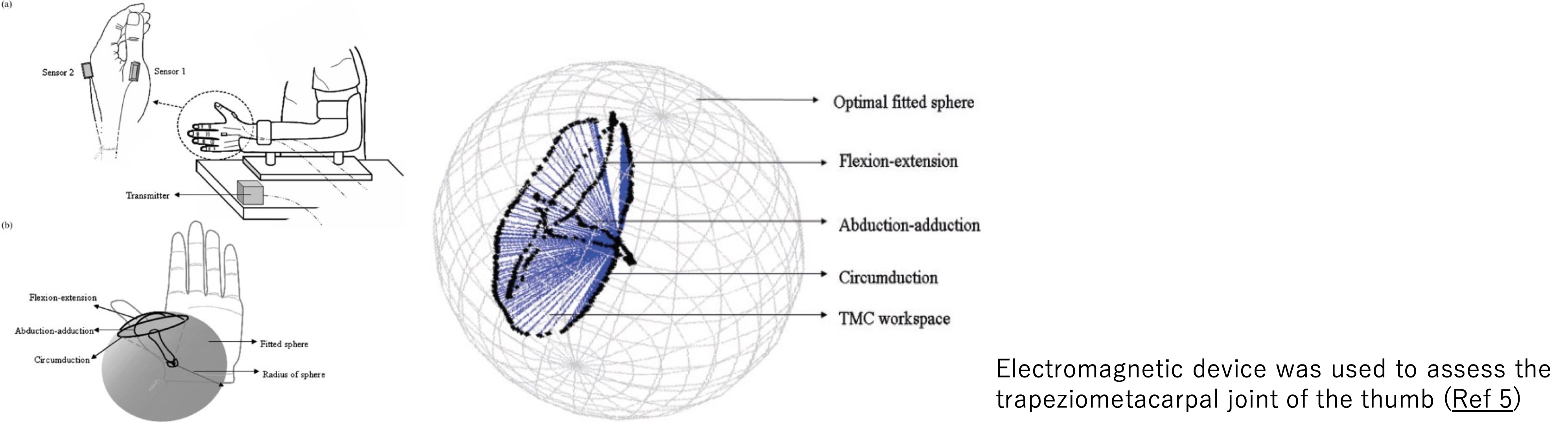
An electromagnetic device, specifically a 3-space device, has been used to assess the trapeziometacarpal joint of the thumb. The space traced by the tip of the first metacarpal joint was measured for comparison (Ref 5).
Video-based motion systems have also been adopted for assessing hand motion. For example, finger movements in piano playing have been evaluated using such a system (Ref 3). The movement of the fingers associated with the rehabilitation of trigger finger has also been studied. A specific movement pattern was found to be beneficial in reducing tendon tightness and improving tendon gliding. In this study, the space covered by the fingertip was also used to assess treatment effectiveness. (Ref 4)
An electromagnetic device, specifically a 3-space device, has been used to assess the trapeziometacarpal joint of the thumb. The space traced by the tip of the first metacarpal joint was measured for comparison (Ref 5).
 2. Joint Articulation Motion
Each joint in the hand has a unique pattern of movement, influenced by the distinct shapes of the articulating bony structures and the capsuloligamentous constraints. For example, the metacarpophalangeal joint has two degrees of freedom: flexion-extension and abduction-adduction (Ref 6), whereas the interphalangeal joints allow for one degree of freedom—flexion-extension. The basal thumb joint, the carpometacarpal joint, has a unique saddle-shaped bony structure that permits universal joint motion (Ref 7).
To meet the high demands for stability in force transmission and to match the shape of objects being manipulated, the wrist joint functions as an intercalated joint consisting of eight carpal bones without direct muscle and tendon attachments. The relative movements among the carpal bones are regulated by the shapes of the intercalated bony structures and the constraints of the intrinsic and extrinsic carpal ligaments (Ref 8). Gross loading across the wrist joint thus affects the relative kinematics of the carpal bones (Ref 9).
3. Joint Constraint and Stability
In general, joints in the hand are flexible, allowing for a wide range of movements. However, when forceful manipulation is required, joint stability is essential to resist muscle contraction and external forces. Joint stability is achieved through the integrated action of dynamic muscle contraction and the compression in the bony articulations and tension of capsuloligamentous structures.
The relative contributions of collateral ligaments to resisting radioulnar forces at the metacarpophalangeal joint have been studied using a “stiffness test” (Ref 10). In this test, the joint is displaced, and the resulting resistance forces or moments are measured. Subsequent sectioning of the soft tissue structures, the reduction of those constraint forces and moments reveals how much each anatomical structure contributes to joint stability. A similar stiffness test has also been used to examine the stability of the proximal interphalangeal joint (Ref 11).
Alternatively, joint stability has been studied using a “laxity test”, where a consistent load is applied, and the laxity of the joint is measured. The contribution of capsuloligamentous structures is assessed through sequential sectioning ( Ref 12). This method has been used to examine the role of the thumb carpometacarpal joint and to assess the integrity of the intercarpal ligaments, particularly in relation to scaphoid-lunar dissociation (Ref 13). Additionally, stiffness tests have been applied to study the rotational stability of the carpus relative to the forearm (Ref 14).
4. Hand Strength
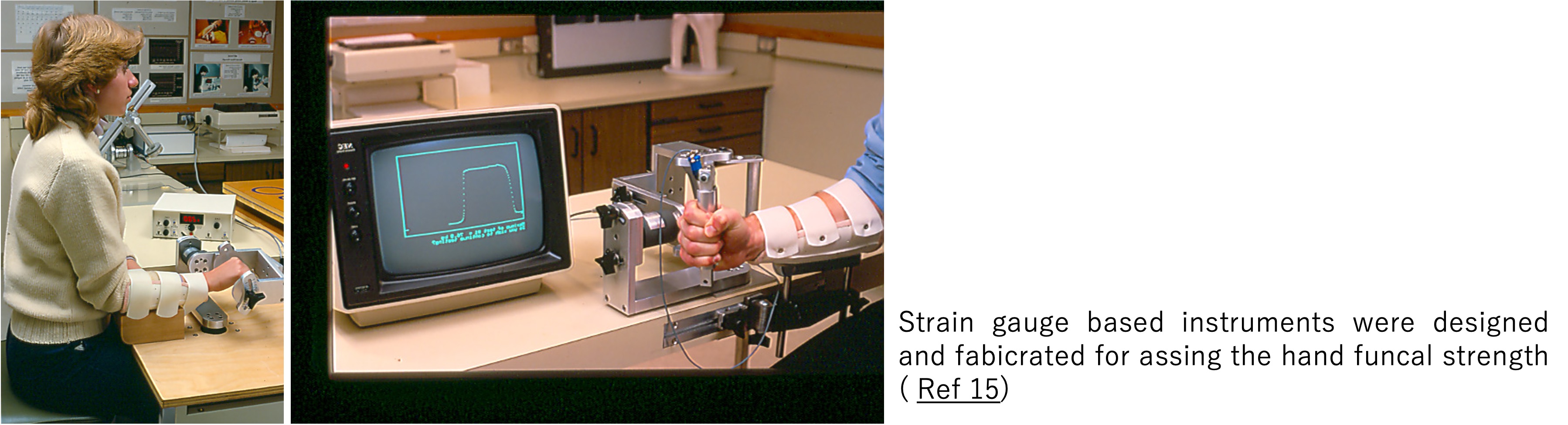
The functional strength generated by the hand—such as grip and pinch strength—can be assessed using dynamometers. Most of these devices are equipped with strain gauge sensors (Ref 15). In grip strength measurements, the forces generated by each of the phalanges of the digits can vary from individual to individual.
2. Joint Articulation Motion
Each joint in the hand has a unique pattern of movement, influenced by the distinct shapes of the articulating bony structures and the capsuloligamentous constraints. For example, the metacarpophalangeal joint has two degrees of freedom: flexion-extension and abduction-adduction (Ref 6), whereas the interphalangeal joints allow for one degree of freedom—flexion-extension. The basal thumb joint, the carpometacarpal joint, has a unique saddle-shaped bony structure that permits universal joint motion (Ref 7).
To meet the high demands for stability in force transmission and to match the shape of objects being manipulated, the wrist joint functions as an intercalated joint consisting of eight carpal bones without direct muscle and tendon attachments. The relative movements among the carpal bones are regulated by the shapes of the intercalated bony structures and the constraints of the intrinsic and extrinsic carpal ligaments (Ref 8). Gross loading across the wrist joint thus affects the relative kinematics of the carpal bones (Ref 9).
3. Joint Constraint and Stability
In general, joints in the hand are flexible, allowing for a wide range of movements. However, when forceful manipulation is required, joint stability is essential to resist muscle contraction and external forces. Joint stability is achieved through the integrated action of dynamic muscle contraction and the compression in the bony articulations and tension of capsuloligamentous structures.
The relative contributions of collateral ligaments to resisting radioulnar forces at the metacarpophalangeal joint have been studied using a “stiffness test” (Ref 10). In this test, the joint is displaced, and the resulting resistance forces or moments are measured. Subsequent sectioning of the soft tissue structures, the reduction of those constraint forces and moments reveals how much each anatomical structure contributes to joint stability. A similar stiffness test has also been used to examine the stability of the proximal interphalangeal joint (Ref 11).
Alternatively, joint stability has been studied using a “laxity test”, where a consistent load is applied, and the laxity of the joint is measured. The contribution of capsuloligamentous structures is assessed through sequential sectioning ( Ref 12). This method has been used to examine the role of the thumb carpometacarpal joint and to assess the integrity of the intercarpal ligaments, particularly in relation to scaphoid-lunar dissociation (Ref 13). Additionally, stiffness tests have been applied to study the rotational stability of the carpus relative to the forearm (Ref 14).
4. Hand Strength
The functional strength generated by the hand—such as grip and pinch strength—can be assessed using dynamometers. Most of these devices are equipped with strain gauge sensors (Ref 15). In grip strength measurements, the forces generated by each of the phalanges of the digits can vary from individual to individual.
 5. Muscle and Tendon Force
The unique anatomy of the hand’s bony structures and soft tissue constraints provide the static framework for hand function. However, the dynamic function of the hand relies on the proper contraction and coordination of muscles through intricate neuromuscular control. Ultimately, the forces generated by the extrinsic muscles in the forearm must be transmitted to the fingertips via the connecting tendons. There are several important biomechanical parameters that describe muscle force generation, the manner of force transmission, and effectiveness of moment generation across each joint.
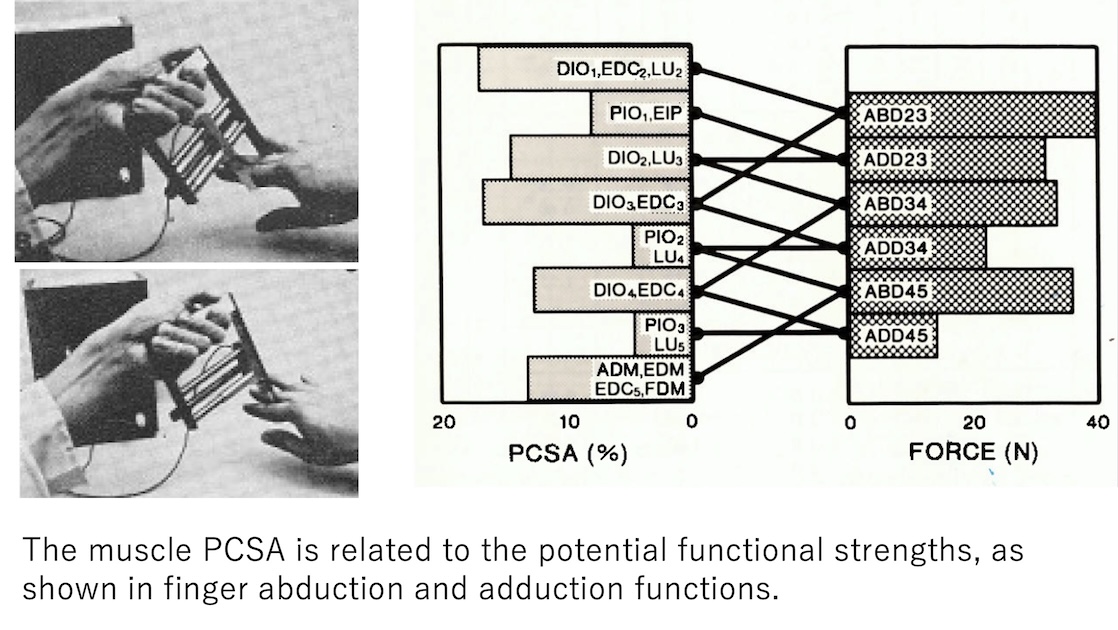
The potential for muscle force generation is related to the size and morphology of the muscle. The “physiological cross-sectional area” (PCSA) of a muscle is commonly used to describe the force that can be generated by that muscle. The fiber length of the muscle indicates the potential for excursion, or the amount of shortening and lengthening that can occur during contraction. Finally, the total volume of the muscle can be associated with the work or energy that the muscle can generate (Ref 16). These muscle morphological parameters have been carefully measured for the intrinsic muscles of the hand (Ref 17). Interestingly, the potential strength of the The fingers is related to these muscles' physiological cross-sectional areas.
5. Muscle and Tendon Force
The unique anatomy of the hand’s bony structures and soft tissue constraints provide the static framework for hand function. However, the dynamic function of the hand relies on the proper contraction and coordination of muscles through intricate neuromuscular control. Ultimately, the forces generated by the extrinsic muscles in the forearm must be transmitted to the fingertips via the connecting tendons. There are several important biomechanical parameters that describe muscle force generation, the manner of force transmission, and effectiveness of moment generation across each joint.
The potential for muscle force generation is related to the size and morphology of the muscle. The “physiological cross-sectional area” (PCSA) of a muscle is commonly used to describe the force that can be generated by that muscle. The fiber length of the muscle indicates the potential for excursion, or the amount of shortening and lengthening that can occur during contraction. Finally, the total volume of the muscle can be associated with the work or energy that the muscle can generate (Ref 16). These muscle morphological parameters have been carefully measured for the intrinsic muscles of the hand (Ref 17). Interestingly, the potential strength of the The fingers is related to these muscles' physiological cross-sectional areas.
 6. Tendon Excursion, Joint Rotation and Moment Arm
The effectiveness of muscle tension in generating torque at the joints, either to move the digits or resist the torque generated by the external forces, depends on the moment arms of the tendon-muscle forces at the joint. The moment arm is geometrically related to the orientation of the tendon’s tension across the joint and its distance from the center of joint rotation. For extrinsic muscles, the long tendons passing through the wrist and digit joints are constrained by pulleys. These pulleys keep the tendons close to the bones as they cross the joints.
In normal anatomy, there is a close relationship between tendon excursion and joint rotation, and the mechanical advantage or moment arm in the following form, The instantaneous moment arm (r) of a tendon can be related to tendon excursion (E) and joint rotation ( φ) as follows:
6. Tendon Excursion, Joint Rotation and Moment Arm
The effectiveness of muscle tension in generating torque at the joints, either to move the digits or resist the torque generated by the external forces, depends on the moment arms of the tendon-muscle forces at the joint. The moment arm is geometrically related to the orientation of the tendon’s tension across the joint and its distance from the center of joint rotation. For extrinsic muscles, the long tendons passing through the wrist and digit joints are constrained by pulleys. These pulleys keep the tendons close to the bones as they cross the joints.
In normal anatomy, there is a close relationship between tendon excursion and joint rotation, and the mechanical advantage or moment arm in the following form, The instantaneous moment arm (r) of a tendon can be related to tendon excursion (E) and joint rotation ( φ) as follows:
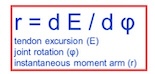 This principle has been confirmed analytically for various tendon-pulley configurations crossing joints (Ref 18).
Experimentally, tendon excursion has been measured using linear or rotary potentiometers in vitro, or via ultrasound imaging in vivo. Joint rotations have been monitored using goniometers, magnetic tracking devices, and imaging systems. The tendon excursion-moment arm relationship has been used to evaluate the significance of pulley constraints and to compare surgical reconstructive procedures, tendon transfers, and reattachments.
The relationship between tendon excursion and joint rotation has been applied to understand the effects of pulley injury and repair (Ref 19). For example, when a pulley is lacerated, tendon bowstringing may occur. This increases the moment arm, which could enhance joint moment generation by muscle force. However, the increased tendon excursion can alter muscle tension generation due to the muscle length-tension relationship. Therefore, proper reconstruction is necessary to restore normal anatomical relationships.
This principle has been confirmed analytically for various tendon-pulley configurations crossing joints (Ref 18).
Experimentally, tendon excursion has been measured using linear or rotary potentiometers in vitro, or via ultrasound imaging in vivo. Joint rotations have been monitored using goniometers, magnetic tracking devices, and imaging systems. The tendon excursion-moment arm relationship has been used to evaluate the significance of pulley constraints and to compare surgical reconstructive procedures, tendon transfers, and reattachments.
The relationship between tendon excursion and joint rotation has been applied to understand the effects of pulley injury and repair (Ref 19). For example, when a pulley is lacerated, tendon bowstringing may occur. This increases the moment arm, which could enhance joint moment generation by muscle force. However, the increased tendon excursion can alter muscle tension generation due to the muscle length-tension relationship. Therefore, proper reconstruction is necessary to restore normal anatomical relationships.
 The tenodesis effect is crucial in the treatment of injuries where tendons cross multiple joints. For example, in the postoperative rehabilitation of flexor tendon injuries, synergistic wrist motion can eliminate tendon slackness in the palm and improve tendon excursion during passive finger joint motion (Ref 20). This motion provides tendon gliding under moderate tension, facilitating healing and reducing adhesion (Ref 21).
7. Joint Forces
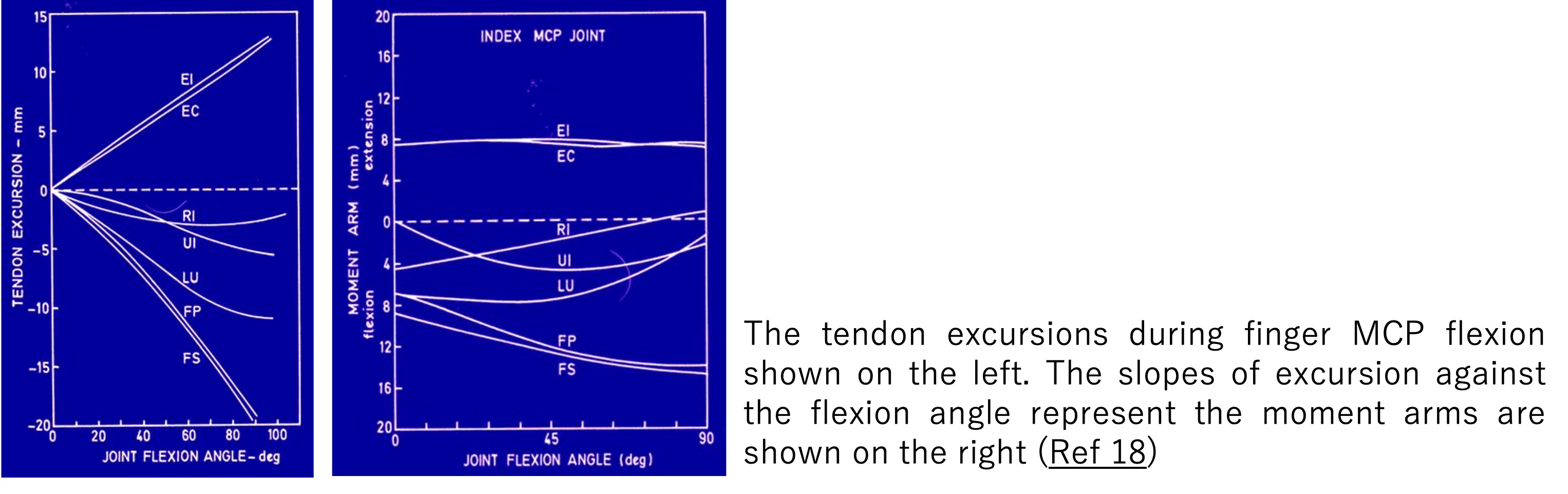
Understanding joint forces is crucial not only for arthroplasty considerations but also for planning treatment modalities and rehabilitation procedures. Direct measurement of joint forces is challenging, if not impossible. Therefore, joint forces are often calculated analytically using mathematical models (Ref 22).
These models are built based on rigorous mechanical principle of free body analysis. In which the anatomical structures are mathematically dissected at the joint and isolated with all externally applied forces and moments preserved. Muscle forces, joint reaction forces, and externally applied forces (such as pinch and grasp forces) are then all factored into the force and moment equilibrium equations. In three-dimensional consideration, such free-body analysis provides six equilibrium equations, three forces and three moments, at each joint. Ultimately, these equilibrium equations are used to solve for unknown variables of muscle and joint forces. However, these systems often become overdetermined, that is there are more unknowns than equations, requiring optimization techniques to resolve the indeterminate problem. (Ref 1)
The tenodesis effect is crucial in the treatment of injuries where tendons cross multiple joints. For example, in the postoperative rehabilitation of flexor tendon injuries, synergistic wrist motion can eliminate tendon slackness in the palm and improve tendon excursion during passive finger joint motion (Ref 20). This motion provides tendon gliding under moderate tension, facilitating healing and reducing adhesion (Ref 21).
7. Joint Forces
Understanding joint forces is crucial not only for arthroplasty considerations but also for planning treatment modalities and rehabilitation procedures. Direct measurement of joint forces is challenging, if not impossible. Therefore, joint forces are often calculated analytically using mathematical models (Ref 22).
These models are built based on rigorous mechanical principle of free body analysis. In which the anatomical structures are mathematically dissected at the joint and isolated with all externally applied forces and moments preserved. Muscle forces, joint reaction forces, and externally applied forces (such as pinch and grasp forces) are then all factored into the force and moment equilibrium equations. In three-dimensional consideration, such free-body analysis provides six equilibrium equations, three forces and three moments, at each joint. Ultimately, these equilibrium equations are used to solve for unknown variables of muscle and joint forces. However, these systems often become overdetermined, that is there are more unknowns than equations, requiring optimization techniques to resolve the indeterminate problem. (Ref 1)
 Generally, muscle and joint forces are found to be three to four times the applied forces at the tip of the finger joint. This is due to the differences in the moment arms of the externally applied forces at the joint center compared to those of muscle and tendon forces.
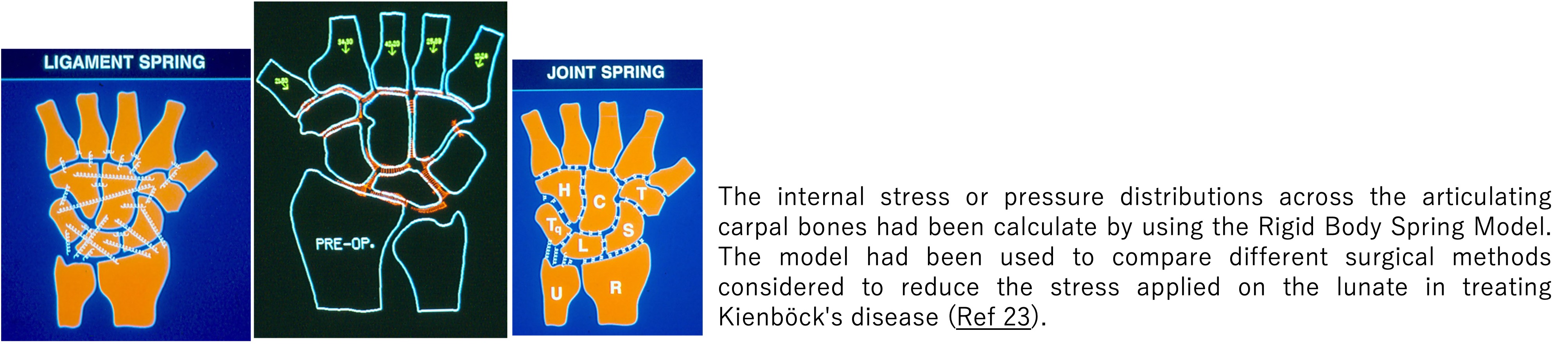
8. Intercarpal Pressure in the Wrist
The distribution of forces across the intercarpal joints in the wrist has been studied to better understand the loading across the carpal boned under normal functions. In addition, the model was used to examine the pathophysiology of wrist disorders and to guide presurgical planning for abnormalities like Kienböck's disease. Several numerical algorithms are used to model this distribution, with one common approach being the RBSM (rigid body spring model), which is a simplified version of finite element models for effective computations (Ref 23, 24). In the RBSM, the bony structures were assumed to be rigid without deformation. On the other hand, the ligaments were represented by tensile springs and the cartilages were considered as compressive springs. The equilibrium equations were then established to balance the internal forces against the external loading, solved for the tensile stress in the capsular-ligament structure and compressive pressures on the joint surfaces.
Generally, muscle and joint forces are found to be three to four times the applied forces at the tip of the finger joint. This is due to the differences in the moment arms of the externally applied forces at the joint center compared to those of muscle and tendon forces.
8. Intercarpal Pressure in the Wrist
The distribution of forces across the intercarpal joints in the wrist has been studied to better understand the loading across the carpal boned under normal functions. In addition, the model was used to examine the pathophysiology of wrist disorders and to guide presurgical planning for abnormalities like Kienböck's disease. Several numerical algorithms are used to model this distribution, with one common approach being the RBSM (rigid body spring model), which is a simplified version of finite element models for effective computations (Ref 23, 24). In the RBSM, the bony structures were assumed to be rigid without deformation. On the other hand, the ligaments were represented by tensile springs and the cartilages were considered as compressive springs. The equilibrium equations were then established to balance the internal forces against the external loading, solved for the tensile stress in the capsular-ligament structure and compressive pressures on the joint surfaces.
 9. Tendon Gliding Resistance
Tendon gliding resistance plays a significant role in hand pathology and treatment considerations. To assess and understand this gliding or friction force, a mechanical model has been developed. A tendon gliding through a pulley can be likened to a belt wrapped around a fixed mechanical pulley (Ref 25). As the tendon moves proximally, the tensions in the tendon segments proximal (F2) and distal (F1) to the pulley are related to the angle (α ) of the tendon segments across the pulley and the friction coefficient (μ) as follows:
9. Tendon Gliding Resistance
Tendon gliding resistance plays a significant role in hand pathology and treatment considerations. To assess and understand this gliding or friction force, a mechanical model has been developed. A tendon gliding through a pulley can be likened to a belt wrapped around a fixed mechanical pulley (Ref 25). As the tendon moves proximally, the tensions in the tendon segments proximal (F2) and distal (F1) to the pulley are related to the angle (α ) of the tendon segments across the pulley and the friction coefficient (μ) as follows:
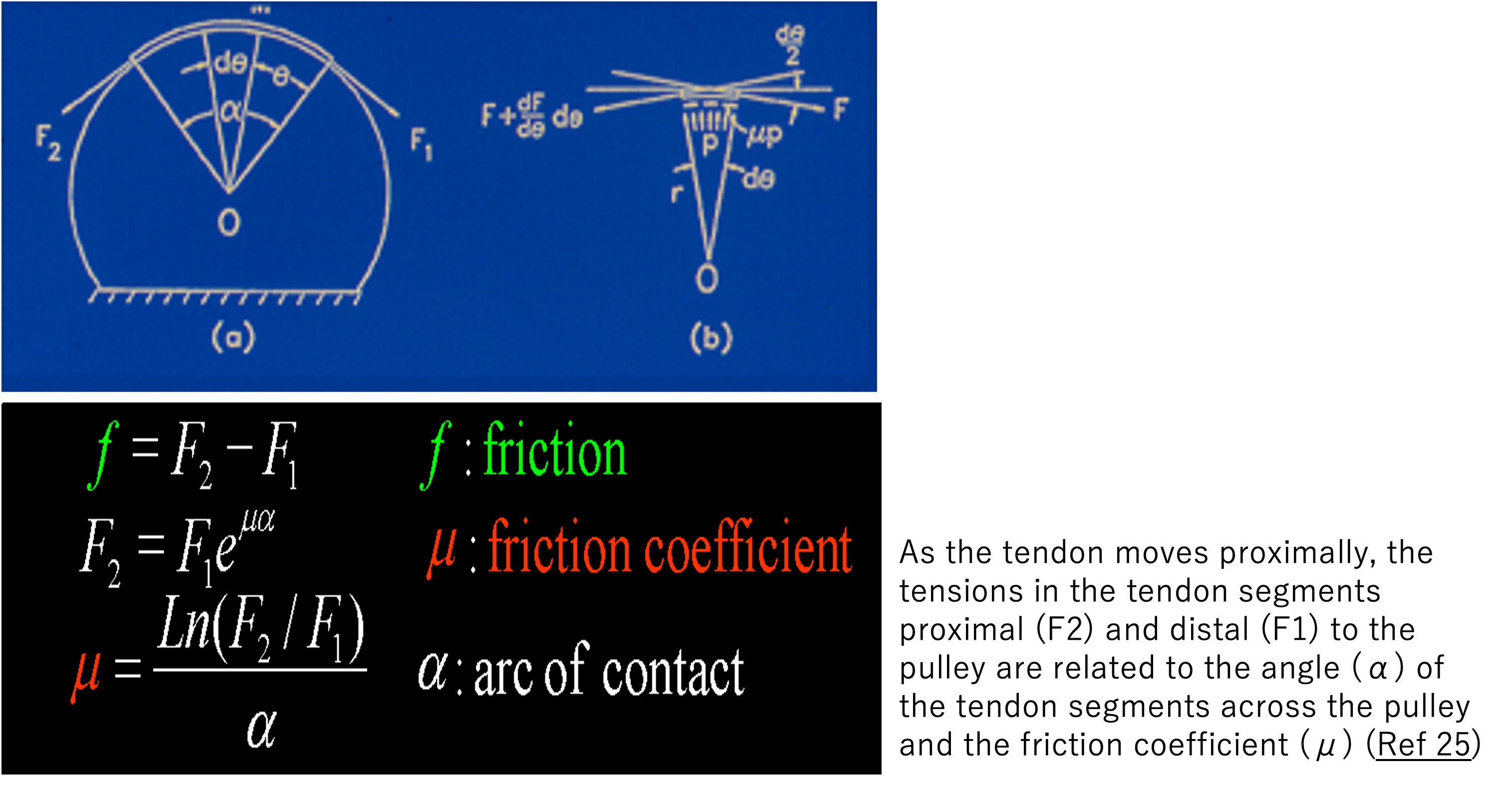 Based on this model, a system was developed to directly measure the friction at the tendon-pulley interface by calculating the difference between F1 and F2. Clinically, this relationship highlights the importance of avoiding awkward joint postures in ergonomic considerations to reduce repetitive soft tissue injuries. In-depth investigations into tendon lubrication mechanisms have provided insight into the potential causes of soft tissue disorders like carpal tunnel syndrome and tendonitis. Clinically, significant improvements have been made in surgical and rehabilitation strategies after tendon repair (Ref 26). This includes the consideration of tendon suture technics, the modification of the tendon graft surface, and synergistic wrist movement in mobilization after tendon repair. The implications for the gliding resistance and friction of the flexor tendons with the surrounding subsynovial connective tissues in the carpal tunnel had been studied extensively to understand the etiology of the carpal tunnel syndrome (Ref 27).
Final remarks:
I am grateful to Professor Mineo Oyama for the kind invitation to participate in the 36th annual meeting of Japan Hand Therapy Society (JHTS), organized by President Koji Horaiya in Nara on April 27, 2024. I thoroughly enjoyed the meeting and will always cherish the fond memories. I hope this paper will be of interest and inspiration to many of you. Please feel free to reach out to me for any further clarification or discussion.
References
Based on this model, a system was developed to directly measure the friction at the tendon-pulley interface by calculating the difference between F1 and F2. Clinically, this relationship highlights the importance of avoiding awkward joint postures in ergonomic considerations to reduce repetitive soft tissue injuries. In-depth investigations into tendon lubrication mechanisms have provided insight into the potential causes of soft tissue disorders like carpal tunnel syndrome and tendonitis. Clinically, significant improvements have been made in surgical and rehabilitation strategies after tendon repair (Ref 26). This includes the consideration of tendon suture technics, the modification of the tendon graft surface, and synergistic wrist movement in mobilization after tendon repair. The implications for the gliding resistance and friction of the flexor tendons with the surrounding subsynovial connective tissues in the carpal tunnel had been studied extensively to understand the etiology of the carpal tunnel syndrome (Ref 27).
Final remarks:
I am grateful to Professor Mineo Oyama for the kind invitation to participate in the 36th annual meeting of Japan Hand Therapy Society (JHTS), organized by President Koji Horaiya in Nara on April 27, 2024. I thoroughly enjoyed the meeting and will always cherish the fond memories. I hope this paper will be of interest and inspiration to many of you. Please feel free to reach out to me for any further clarification or discussion.
References
第36回日本ハンドセラピィ学会学術集会 会長 蓬萊谷耕士
This content summarizes Dr. Kai-Nan An's lecture delivered at the 36th Annual Meeting of the Japanese Society of Hand Therapy. At Dr. An's request, we've created a dedicated website to share this valuable information with hand therapists throughout Japan. While Dr. An has granted permission to publish all papers, due to copyright considerations, we provide direct links to freely accessible papers on our website and bibliographic citations for those requiring purchase. We encourage hand therapy specialists to take full advantage of this exceptional educational resource.
The 36th Annual meeting of the JHTS,President, Koji Horaiya
“Is the Biomechanics in your toolbox?”
Kai-Nan An
Mayo Clinic, Rochester, MN 55901 USA
